The NHS is currently grappling with a growing demand for Dermatology. Waiting lists have grown by 82% since 2021, and the rate of GP referrals for skin cancer having nearly doubled in the last decade. This is compounded by a national shortfall in dermatologists as vacancies in 2021 amounted to 159 WTE. Our report, published in July 2024, has shown that AI holds considerable promise for skin cancer pathways including improving effectiveness and reducing wait times.
AI is currently in use for diagnosis within NHS skin cancer pathways with all lesions second-read by a clinician. Greater efficiency, speed of diagnosis and clinician time could be released if AI as a Medical Device (AIaMD) functioned autonomously. NHS England commissioned Edge health to conduct an independent review of the safety and effectiveness of AI in Dermatology and assessment of its performance against accepted standards of accuracy.
Methods and Key Findings
We examined real-world data from over 33,000 lesions assessed by DERM – an AIaMD developed by Skin Analytics, the only product that currently meets regulatory standards for autonomous use. We conducted a semi-systematic meta-analysis reviewing 153 studies and interviewed eight members of staff across three providers currently adopting the AIaMD. This enabled a grounded perspective on its application in skin cancer detection.
Our findings indicate that DERM’s diagnostic accuracy in ruling out melanomas is at least as good as in-person consultations with dermatologists. This suggests that AI could play a crucial role in distinguishing benign from concerning lesions, streamlining referrals, and ensuring those in need of urgent care are seen promptly. We also identified potential system-level efficiencies, finding that each pound spent could return up to £2.3 in savings. In this context, our report highlights AIaMD’s potential to refine the triage process, thereby addressing the rising demand for services and reducing waiting times for assessments.
While our economic analysis suggests potential savings, the primary focus of the report is on the clinical and operational implications of AIaMD, and what steps should be taken to monitor its use in Dermatology through post-market surveillance (PMS). Clear PMS plans and agreements need to be in place, with responsibilities lying with both deployment sites and manufacturers. Our report condenses PMS recommendations from several literature sources and offers an example of how PMS could be implemented in practice.
The report makes clear that the use of AI holds considerable promise for improving the efficiency and effectiveness of skin cancer pathways. Evidence of its deployment in the NHS has demonstrated that whilst the tool could be used autonomously to exclude benign skin, adequate safeguards, will need to be in place. This provides the potential to free up specialists to focus their expertise on the most urgent and complex cases.
Julia Schofield, Clinical Lead for Dermatology for the National Outpatient Recovery and Transformation programme
Read Our Report
The report concludes that thoughtful deployment of AI in Dermatology has the potential to enhance patient pathways and alleviate system pressures. With appropriate safeguards and continuous evaluation, AI can support the NHS in upholding its commitment to innovative, high-quality patient care.
Finding cancer early is the single biggest step we can make to improving patient outcomes and saving lives. In 2023 just 57.6% of staged cancers[1] were diagnosed at an early stage[2]. This is well below the NHS Long Term Plan ambition of 75% by 2028.
With just 1 in 15 cancers diagnosed via screening, improving early diagnosis is heavily reliant on symptomatic pathways. In practice, this means supporting patients to present early in primary care and supporting primary care to make appropriate referrals through Urgent Suspected Cancer (USC) pathways.
We have partnered with RM Partners, the Cancer Alliance serving North and South West London, to identify practical steps which can be taken in primary care to improve rates of diagnosis. The research is based on analysis of 46 interviews with GPs across West London alongside data including referral behaviour, workforce and population demographics.
The research identified six actions for general practice to increase early diagnosis:
Reviewing practice performance and operation: Understanding and reviewing cancer performance data, participating in cancer audits, internal case review and knowledge sharing.
Adopting quality systems: Use of best practice decision support and safety netting tools, underpinned by a culture of quality improvement.
Addressing systemic inequity: Increasing awareness of systemic inequity and the impact on cancer through training and actively implementing best-practice process.
Workforce stability: Retaining staff without high reliance on locums, whilst ensuring clear orientation of locums when required.
System awareness and participation: Awareness and use of direct access and Vague Symptom pathways, building relationships within PCNs and with secondary care
Training and clinical improvement: Accessing cancer-specific training to support the appropriate use of cancer pathways.
These findings are underpinning the support being provided to primary care teams within RMP. More detail on the research findings and recommendations as well as the methodology can be found below, and both reports are available to download.
Since the pandemic, SACT activity has grown rapidly
The number of patients receiving Systemic Anti-Cancer Therapy (SACT) in Thames Valley grew by 7% between 2021 and 2022. This rise in activity, combined with increasing treatment complexity, length, and national shortages in SACT staff, has put pressure on departments and workforce.
Thames Valley Cancer Alliance serves a population of 2.3 million people, spanning two ICSs, four Acute Trusts and nine Hospitals. SACT is delivered within the Alliance by Oxford University Hospitals (OUH), Buckinghamshire Healthcare (BHT), Royal Berkshire (RBH) and Great Western Hospitals (GWH).
Starting in September 2023, Edge Health worked closely with TVCA and its constituent trusts to provide demand and capacity analysis, identify system pressures and develop innovative solutions to meet this need over the next five years.
As an Alliance, we were aware of the national and regional SACT pressures and wanted to review our demand, capacity and workforce to support service development and raise the awareness of the significant increase in activity we will expect in the coming years. Edge Health worked closely with our clinical teams to understand the pressures and activity in SACT services and to provide recommendations to be delivered across the system including a demand and capacity tool for our biannual SACT assessments.
Edge Health are knowledgeable, professional and a very approachable team supporting the requirements of our service.
Lyndel Moore – TVCA Cancer Clinical Lead for Nursing and AHPs
Our approach involved working closely with key stakeholders across the Alliance to draw out insights from provider data and workforce interviews
After gathering data on patient volumes, complexity and treatment types and combining this with workforce data from all four acute trusts, we interviewed key clinicians and stakeholders to understand and articulate the pressures and problems that they were facing on a day-to-day basis.
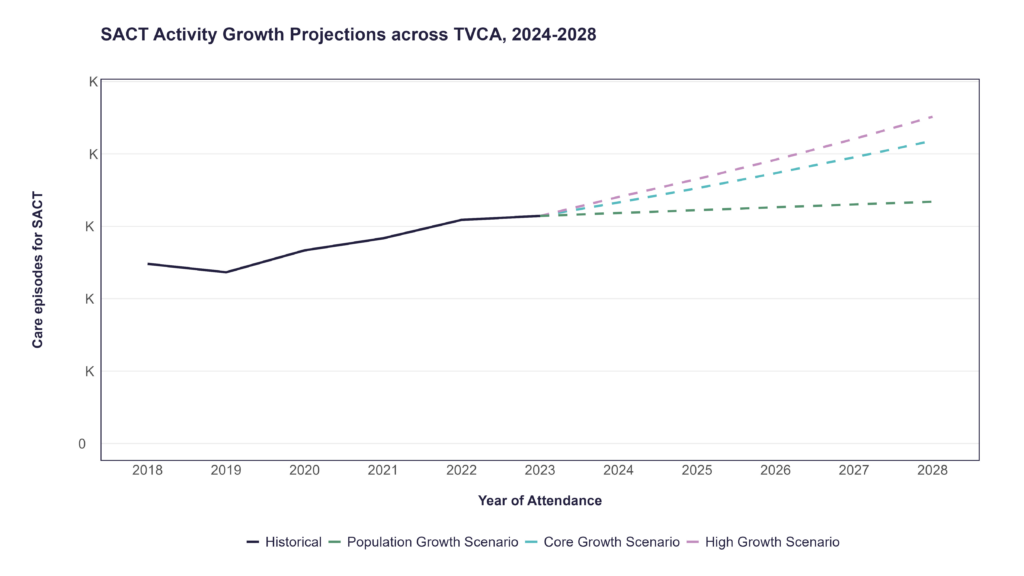
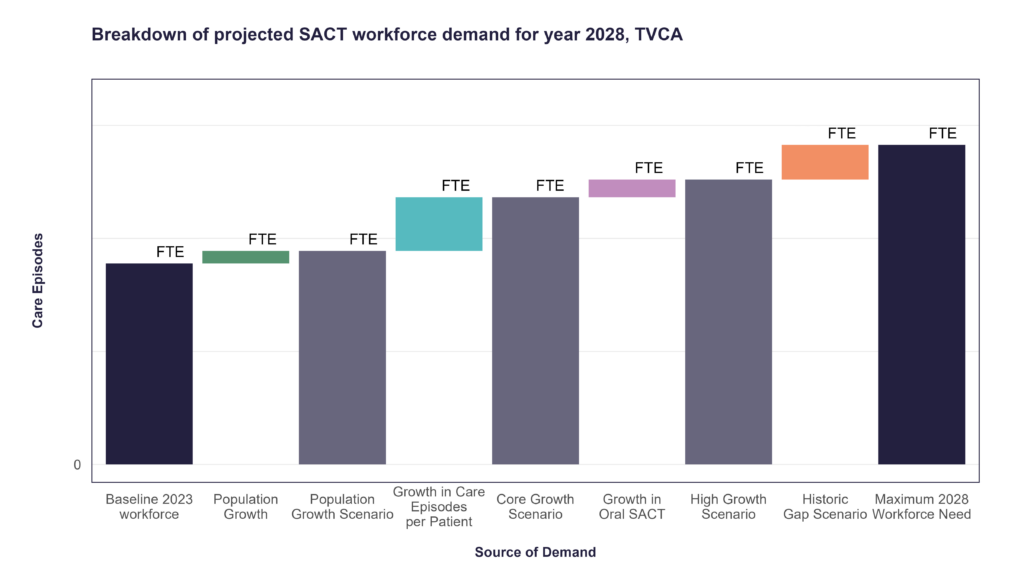
From data and interview insights, we developed a set of scenarios for the future growth of SACT treatment within the alliance. These were:
Population growth scenario: demographics-driven model
Core growth scenario: based on growth trends observed locally and nationally
High growth scenario: accounting for additional pressure exerted by factors such as high growth in demand for oral SACT treatments
Note: Chart figures hidden for confidentiality
We wanted to provide actionable solutions to pressures faced by SACT units
Engagement with trusts and thorough analysis led to the identification of four wide areas for opportunity:
Capacity
Efficiency
Workforce
Operations
We developed creative and practical opportunities that Trusts could utilise to help tackle these growing problems, such as increasing self-administration of subcutaneous SACT to manage capacity pressures or developing non-administrative and managerial professional growth avenues to help increase the retention of workforce.
To aid Trusts with their future demand and capacity planning needs, we produced an interactive demand model. This allows Trusts to use pre-generated demand projections or input their own figures for future workforce planning and has already been used as part of TVCA’s bi-annual demand and capacity planning.
Waiting List Modelling: Effectively Achieve Elective Targets
Meeting national targets for elective treatment in the wake of COVID-19 has been challenging for Trusts across England
The impact of Covid-19 on the delivery of elective services has been substantial: waiting lists have built up, with a sizeable backlog of patients waiting longer for treatment than ever before, and referral volumes have returned to levels which exceed the pre-pandemic norm.
Trusts must deliver NHSE expectations around waits to treatments and sizes of waiting lists, and to do this need a robust understanding of required capacity and efficiency levels, as well as the impact of future known interventions and referral volumes.
Staring in November 2022, Edge Health worked with Leicester, Leicestershire and Rutland (LLR) Integrated Care Board to support with operational decision-making and elective care planning to meet these targets.
Our approach involved working closely with system leadership in LLR to draw out insights from acute, community and primary care provider data
Our objective was to support stakeholders to clearly articulate the gap between current capacity, demand and delivering NHSE targets, to a range of audiences and forums. This allowed the system to proactively identify areas of pressure, develop a plan and set of scenarios and track progress relative to expectations.
Using simulation modelling and demand forecasting techniques, we built a robust understanding of the impact of system-wide interventions on waiting list projections. We proactively identified areas of pressure and followed up with demand & capacity deep-dives for 4 specialties and 9 diagnostic modalities.
The outcome was drastically improved waiting times to elective treatment, following informed, evidence-based system and Trust-level leadership and investment decisions
The sole acute provider in LLR improved from being 3rd worst-performing Trust for 92nd percentile waiting times and proportion of patients waiting over 65 weeks for elective care, into the top 50% of Trusts for both measures[1]. Total waiting list size has plummeted, with LLR on-track (again in the top 50% of Trusts) to meet the March 2025 target of no patient waiting over 1 year for treatment.
Our analysis provided the evidence base to support LLR system and Trust-level leadership with cohesive decision-making and strategic planning for the future. We helped a range of stakeholders to understand risks and focus on the most likely scenarios, and the scale of intervention and investment required to proactively reduce pressure on elective services.
As of November 2023, the NHS faced a significant challenge with approximately 7.61 million patients on waiting lists for various treatments. This figure underscores a critical issue within the healthcare system, highlighting both the clinical risks associated with delayed follow-ups and the operational strains on healthcare resources.
Addressing Waiting List Challenges with PIFU
The concept of Patient Initiated Follow-Up (PIFU) has emerged as a strategic response to these challenges. By allowing patients to determine the necessity and timing of their follow-up appointments, PIFU aims to enhance patient safety, optimise appointment scheduling, and reduce unnecessary follow-up engagements, thereby potentially decreasing waiting list volumes.
Despite the theoretical benefits of PIFU, there remains a lack of empirical evidence supporting its efficacy in practice. This, along with the ever-present challenges of changing existing pathways, means that many Trusts will miss the modest target of moving 5% of outpatient attendances to PIFU pathways, that NHS England set for March 2023 as part of the Elective Recovery Strategy.
The Role of DrDoctor and Key Findings: up to £167 million in System-wide Savings
In this context, DrDoctor, which oversees around 20% of NHS outpatient booking activities, including PIFU services, has played an important role. Through its operations across multiple Trusts, DrDoctor has gathered extensive data that, when analysed alongside Trust-specific data, offers insights into the potential health economic benefits of PIFU to inform increased usage and improvement of the service.
Edge Health was commissioned by DrDoctor to combine learning from this data as well as from interviews with clinical and operational staff involved in implementation at two large NHS Trusts to start evaluating this service delivery model. The report sets out the findings from data analysis, literature review and operational and clinical engagement into the potential real-world benefits, and best practice implementation of PIFU.
Key findings suggest that achieving the national target of a 5% PIFU pathway adoption rate could result in the saving of approximately 1,393,154 outpatient follow-up appointments annually, leading to an estimated system-wide saving of at least £167 million, based on 2020/21 figures.
Implementation Insights and Potential Impacts
Our report also provides details on how to effectively implement digital PIFU within Trusts, based on conversations with implementation teams. This highlights the types of specialties proven to be most successful to date, the conditions for the successful delivery of the roll-out of digital PIFU, key challenges services faced with implementation and what learnings they would give other Trusts at the start of their implementation.
The report also highlights the benefits to patients and the NHS of another form of patient-initiated pathway, Patient Initiated New Appointment (PINA). This is where patients referred to secondary care for an appointment are given control over whether they still require the appointment.
This report provides invaluable, real-world evidence highlighting the extensive value of implementing PINA and PIFU at scale within the NHS. It underscores the transformative role digital tools have in simplifying processes, modernising patient care and driving efficiency of system operations. We’re pleased to have worked with EDGE Health in producing this report and are excited about the wider impact this collaboration will have on the healthcare sector in reducing unnecessary follow-up appointments and tackling the backlog.
Tom Whicher, CEO of DrDoctor
From a waiting list perspective, PINA can help reduce the number of unnecessary first appointments at a Trust, in a similar way to PIFU. It is estimated that between 3-15% of patients on the waiting list do not need an outpatient appointment by the time they get contacted. By removing eligible patients who do not actually need a first outpatient appointment and are appropriate for PINA, our report found that the waiting list significantly decreases. This could mean a reduction in the waitlist by between 228,000 and 1,141,500 patients.
Therefore, the findings from our report can be used by Trusts to understand the potential of patient-initiated appointments (both PINA and PIFU) at their Trust and help them meet NHS England targets, while also driving down waiting list size and improving patient experiences.
AI-Teledermatology: Innovating Skin Cancer Diagnostics
The healthcare system in England and Wales is experiencing unprecedented pressure due to the sharp rise in demand for dermatology services. With one in four individuals seeking consultation for skin, hair, or nail conditions each year, the need for innovative solutions has never been greater. The COVID-19 pandemic exacerbated this strain, causing a 30% drop in dermatology appointments during 2020/21 and a subsequent surge in patient referrals post-pandemic, with suspected cancer referrals rising 13% nationally compared to 2018. Rising volumes of urgent suspected cancer referrals have significant impacts for system sustainability – under a strained system, they correlate with higher volumes of patients breaching care standards, such as the 62-day treatment standard, as explored in a previous piece of work.
The potential of teledermatology, particularly AI-powered teledermatology, has been recognised as a promising solution to expand service capacity and ensure equitable patient access to specialist care. The Skin Analytics AI-Powered teledermatology for Skin Cancer 2-week-wait (2WW) Pathway was pilot tested across University Hospitals of Leicester (UHL) sites starting from March 2022. This collaborative project was designed to respond to the local need for improved patient access to dermatology diagnostics and the achievement of 2WW cancer targets.
Our evaluation underscored the potential of AI-powered teledermatology. Despite being in its pilot phase, the AI tool demonstrated its capability to enhance patient access to dermatology services. While the initial benefit-cost ratio stood at 1.05, this figure doesn’t fully encapsulate the unquantified benefits, such as a reduction in biopsies, long-term care costs, and WLI clinics. Workforce costs were also front-loaded prior to capacity being fully utilised, leaving room for a higher benefit-cost ratio.
The current pathway model relies on second-reads to be performed on all AI-screened scans, with a further reduction in the potential benefit-cost ratio as well as increased pressure on clinical teams. In our evaluation, the AI outperformed documented clinical diagnostic standards[1], but our staff survey highlighted current reservations from consultants in dispensing of the second-reads altogether.
The evaluation also supported the health system through highlighting potential administrative challenges that scaled expansion would need to monitor for. These included timely booking of appointments for patients on the novel pathway, as well as ensuring that commissioning arrangements reflect the true costs of providing an innovative service – and are aware of the prospected savings.
Scenario Modelling for Future Savings
Looking ahead, we conducted scenario modelling to explore the potential for greater savings in the future. These scenarios hinge on reducing or removing the cost associated with the second read of dermoscopy images, leading to a benefit-cost ratio ranging from 1.3 to 1.9.
Our evaluation indicates that this novel pathway could be cost-effective in the long term. It could also offer considerable benefits to the wider Dermatology cohort, healthcare staff, and the health system if implemented at scale, with potential yearly savings across the Midlands ranging between £2.1M and £5.7M, depending on who performs the second read.
Recommendations for Enhancements
As part of our commitment to continuous improvement, we proposed several recommendations. These include streamlining administrative processes, evaluating the best option for lesion second reads and conducting further evaluations as the AI versions improve and more data becomes available.
Our work with Health Innovation East Midlands, UHL and Skin Analytics demonstrates Edge Health’s commitment to pioneering innovative healthcare solutions. Evaluating the effectiveness of new technologies such as AI-powered teledermatology is a fundamental step in improving services so that they are accessible, efficient, and patient-centred.
Our overall experience of working with Edge was very positive, and their analysis and evaluation process was robust and innovative. They handled challenges well and always sought a balanced solution with cross-stakeholder agreement. The Final Report was delivered on track and met the expectations outlined in the original scope and MOU.
Michael Ellis – Senior Innovation Lead, Health Innovation East Midlands
Key Successes
Conducted a comprehensive independent evaluation of the AI-powered teledermatology pilot initiative.
Identified potential for significant future savings through scenario modelling.
Proposed actionable recommendations to enhance the programme’s benefits and ensure long-term cost-effectiveness.
Highlighted the importance of considering administrative implications of implementing novel technologies.
Provided insights to guide future evaluations as AI technology evolves and more data becomes available.
This project was carried out in partnership with Health Innovation East Midlands
Full Report
The evaluation report can be accessed on the Health Innovation East Midlands website, as well as previewed below.
[1] Chuchu N, Dinnes J, Takwoingi Y, Matin RN, Bayliss SE, Davenport C, Moreau JF, Bassett O, Godfrey K, O’Sullivan C, Walter FM, Motley R, Deeks JJ, Williams HC. Teledermatology for diagnosing skin cancer in adults. Cochrane Database of Systematic Reviews 2018, Issue 12. Art. No.: CD013193.
A Data-driven Approach to Planning Radiotherapy Workforce Requirements
There is no greater source of pressure in the NHS at the moment than staff shortages. Rising demand, growing complexity and lengthening waitlists, combined with high turnover, absence and staff leaving the NHS post-Covid, have created a gap between demand and supply of staff.
Understanding and responding to this gap is a complex problem across the health system. Doing so requires a detailed understanding of future workforce requirements and innovation in model and roles. By partnering with Dearden HR, award winning HR and OD consultants, we are able to combine our robust analytics and understanding of data with bespoke people and OD solutions.
West London, Surrey & Sussex Radiotherapy Operational Delivery Network
One example of our work together was with the West London Surrey & Sussex (WLSS) Radiotherapy Operational Delivery Network (ODN). The ODN, which comprises 4 radiotherapy providers, sought to understand their future workforce requirements and opportunities to innovate and implement a new workforce model to meet demand.
Approach
Our approach revolved around three workstreams. The first two supported the development of a rich evidence base, through modelling of future demand and activity and gaining a detailed understanding of the ODN’s current workforce status. These efforts formed the groundwork for assessing the future workforce requirement and developing an action plan for meeting this requirement. Our approach was designed to ensure that the final outputs are rigorous in detail and evidence, innovative in approach, built off existing best practice and co-developed with providers and ODN leadership.
The modelling was built on anonymised attendance-level data collected from each provider. This level of detail allowed for robust modelling of the workforce requirements of current and future activity, considering changes in complexity, treatment type and pathway. This was supported by workforce data and staff engagement, including a questionnaire and interviews to better understand each Trust’s workforce model, as well as staff motivation and job satisfaction at each of the Trusts. This multi-faceted approach ensured a comprehensive understanding of the present workforce landscape and laid the groundwork for informed workforce planning and recommendations.
Future demand was modelled based on a range of scenarios, considering changing population, demographics, population health and cancer treatment. This modelling informed future workforce requirement scenarios. An interactive workforce planning tool was developed alongside the final report, enabling scenario analysis for future workforce shortfalls or surpluses based on Trust-specific assumptions.
“Partnering with Edge Health allows us to develop recommendations and an implementation plan which is based on clear and rigorous data analysis.”
Michelle Hodgkinson, Director, Dearden HR
Outputs
Based on the demand and capacity modelling and our understanding of current staffing levels, we calculated the additional establishment and in-post WTE required to meet the recommended level of staffing. The work also developed a series of recruitment and retention interventions, including regarding:
Apprenticeships
International recruitment
Active retention and support
Development roles
Flexible working
The combination of quantified workforce gaps and recommended interventions has provided the ODN and each Trust with a strategy for addressing future workforce pressures. This is currently being taken forward within the ODN.
Routine orthopaedic procedures are more complex than ever before in the NHS
A decade of Staffing shortages, low bed capacity and a devastating 2-year pandemic has culminated in an unprecedented backlog of elective procedures for the NHS with over 7 million patients currently waiting for care in England1.
As a response to these growing waitlists, the NHS conceived the national high-volume low-complexity (HVLC) programme during the COVID-19 pandemic. This programme has worked to standardise pathways, introduce surgical hubs, and improve theatre productivity to increase the throughput of trusts performing routine procedures. It has long been suspected however, that routine procedures in the NHS are not as low complexity as they were before the pandemic2. This is in part due to increasing prevalence of long-term illnesses3, an ageing population4, and the degradation of patient health whilst waiting for surgery2.
As part of our work supporting the GIRFT HVLC programme, we have worked with surgeons to identify patient characteristics that have statistical relationships with the cost of high-volume orthopaedic surgery procedures. These include clinical diagnoses, such as cancer or diabetes in patient records, procedural features, such as the emergency admissions prior to surgery, or patient demographics, such as age and deprivation. Using Machine Learning approaches, we can quantify the impact of these features and develop an indicator of clinical complexity in routine procedures. Our work brings light on the poorly understood impact of increasing patient complexity and is the first step towards mitigating and tackling the increased burden being felt by surgical specialties in England.
Methodology
To quantify patient complexity, 2 key data sources have been used.
Hospital Episode Statistics (HES), a detailed dataset containing clinical, demographic, and patient information.
Patient Level Information and Costing Systems (PLICS), a dataset relaying the cost of hospital admissions in England.
By linking these two sources, we have been able to create statistical models that uncover the relationship between clinically relevant patient features and the cost of a procedure. Specifically, we have worked with Orthopaedic surgeons to select 22 drivers of operation cost which are shown in Figure 1.
Figure 1. Features used to estimate clinical cost from HES data.
HES/PLICS data from 2018-19 was used to extract these features and train procedure specific linear regression models that estimate procedure cost. Using these models, we can track the estimated cost that is driven by the clinical characteristics of the patient over time which is a pertinent indicator of patient complexity.
Findings
The expected costs have been calculated for 3 major HVLC orthopaedic procedures in Figure 2. They clearly show that since the COVID pandemic, patients have been more complex and resource intensive than ever before. Analysis of patients has revealed this increase is primarily driven by increased frailty, as there is a 30% increase in patients with a severe frailty score, as well as a 10% increase in the average number of significant ICD-10 codes. Worryingly, this increase shows no sign of reversing as of March 2023, suggesting that this trend is potentially here to stay.
This work reveals several far-reaching implications for the NHS, most notably that routine procedures are likely to drain resources more rapidly than ever before. Unless hospitals are paid accurately to reflect these changes, there will be a reduction on how much can be spent on staffing and other resources which further damages patient care. We have compiled a set of key recommendations that aim to mitigate the knock-on effects of complexity increase.
Increased cost and resourcing requirements should be reflected when creating activity plans. This will affect trust, care system and specialty managers with limited budget.
Tariffs should be regularly updated to reflect the ever-changing patient case mix that is seen by hospitals. The tariffs should also be sensitive to demographic features of patients, such as age and deprivation, as we have found that these are important drivers of surgery cost.
Programmes should focus on increasing the general health of patients before elective admission. We have shown that the increased expected costs of hip replacements alone amount to over £13 million pounds per year for the NHS. If programmes, such as the PREP-WELL project by the health foundation5, can demonstrate that they are able to reduce clinical complexity, there is large potential for savings.
National programmes that track surgical outcomes, such as Model Hospital and the National Consultant Information Programme, should adjust performance metrics to account for changing patient case mixes. This will enable increased buy in from clinicians who have been most directly affected by increased complexity.
The focus for efficiency gains has traditionally been on theatres, inpatient and outpatient activity and more recently the growing elective backlog. Diagnostics, however, have acquired a new emphasis since COVID. This is because significant backlog in diagnostics is causing delays in finding cancers (you can read more about this on our blog).
As a response, NHSE has included diagnostics activity targets in the NHS Constitution, stating that all tests must be performed within 6 weeks from request. This puts pressure on trusts to understand their testing activity, capacity and bottlenecks in imaging reporting that cause downstream delays in the 18-week referral to treatment (RTT) target.
Trusts have not historically analysed diagnostics data in depth
Gathering these insights requires analysis and data flows which are not yet set-up well across Trusts. Data from radiology information systems (RIS) has not been used as extensively in the past and existed in lower quality than, for example, theatre data. In this context, Trusts now struggle making sense of their imaging data to action NHSE targets.
We were recently asked to support a large specialist NHS Trust in helping with this.
The ask: time-sensitive solutions to guide management
We did this in three stages:
Analyse national data to get a high-level picture.
Engage with team on the ground to understand what actionable insights are needed where and why they are not provided.
Deploying expert clinicians and analysts to provide the insight in a repeatable way.
We outline each of the below in turn and give some detail on the issues under the hood.
First: Public data
First, we explored publicly available data on the Trust’s diagnostics to form the start of meaningful conversation and gain a high-level understanding of some of their challenges. The two charts below showed that our client (Comparator 1 in the chart on the left) had above average waiting times for a scan to be reported, following testing. The time between testing and reporting had also seen a significant increase in 2022/23 compared to 2019/20, particularly for MRI, Nuclear Medicine and Single Photon Emission CT.
Second: Working with team on the ground to understand the problems
We then sat with stakeholders to map the imaging data journey at the Trust and uncovered the key issues within it (outlined below).
Issues we found were the below:
Complicated set-up: Before an end-user could reach any insight, four pieces of software needed to interact: a requesting software like ICE, a RIS software, a PACS software and finally a BI software, QlikView in the client’s case. All insights needed to wait till the analytics team had curated the data.
No quick way around it: Managers trying to extract data from RIS directly were faced with a complex interface that was both hard to work with and at risk of producing unreliable metrics. This step was incredibly time-consuming for managers, adding to undue stress.
Lack of resources: There were no dedicated imaging analysts at the Trust, which meant the imaging team had to compete with other teams to get the insights they needed from the busy BI department.
We supported the trust outlining a variety of solutions, including:
Increasing workforce, such as a specialist PACS or analytics team member.
Changing work practices, such as setting a cap on highly time-consuming MDT requests to focus on internal workload, and upskilling radiographers to report imaging.
Upgrading software to one that included basic analytics, timed with a contract soon to expire.
In order to tie the department over with an urgent need for insights, we also delivered a fast turn-around reporting solution ourselves, embedded in their current BI environment.
Third: Delivering a trusted solution
We were onboarded on the Trust’s system to work within their environment and built a relationship with the BI and analytics team to ensure seamless knowledge transfer and accuracy of outputs.
Engaging with stakeholders also helped build trust in the outputs and ensure that it was truly useful to the team and met expectations.
Early draft of one of our reporting interfaces showing high-detail overview of reporting activity by radiologist and imaging modality, and reporting waiting times at a glance.
By the time the tool was ready to be shared Trust-wide, it had received the seal of approval from the imaging manager, the clinical director, and the BI lead. The final product was fully handed over to the Trust’s BI team to use as a starting point for more analysis and maintain as required in the future.
Specifically, it provided a high-detail overview of reporting activity by radiologist and imaging modality, and reporting waiting times at a glance.
This is enabling the Trust to:
understand pressures on the imaging department
manage workflows more effectively
back department investments and business cases with evidence
improve their performance against NHS diagnostic targets.
 Back to News & Insights
Back to News & Insights