Advancements in machine learning have led to the rise of pre-trained Large-Language Models (LLMs) that can be used to interpret, understand, and process medical data. As a demonstration of this technology, we have built a proof-of-concept (POC) tool that transforms unstructured and doctors’ notes and chest x-rays into a structured database.
What is the opportunity for healthcare providers?
According to some studies, up to 97% of medical data sits unused within hospital premises. This is a huge untapped resource that could help providers optimise pathways, improve patient care and unlock financial gains through better coding and saving clinical time.
The main downside, however, is that much of this data sits in unstructured formats, such as images. Extracting meaningful data from these can be time consuming and expensive, but our proof of concept demonstrates how the latest AI developments could overcome these barriers, allowing greater utilisation of data for hospitals.
Proof of concept using chest X-rays
Our tool harnesses a state-of-the-art open-source pretrained language model (Zephyr-7B) and an image to text model that extracts information from DICOM images (llava-1.5-7b). We have tested the feasibility of our approach by applying it to the MIMIC-CXR public dataset of chest X-rays and doctors’ notes.
Our POC is able to reliably take this complex data source, which contains rich medical information, and distil the details into predetermined fields of a table, leading to a simplified version of the original dataset.
Processing pipeline for X-Ray images and doctor’s notes.
Why are structured tables, such as knowledge graphs, more useful than their unstructured counterparts?
By compressing rich clinical information into salient indicators and storing it in tables, we can create structured datasets that relay important details about patient care, such as their diagnosis, procedures and outcomes.
In turn, researchers, auditors, and clinicians can easily draw insights from large numbers of patients using simple data analysis approaches, allowing them to understand how interventions impact patient outcomes and determine methods to improve patient care.
Transformed knowledge graph output from the discharge notes and multiple X rays of a single patient.
Plenty of use cases
A tool like this could be employed to validate secondary-use datasets which are currently manually created by clinical coding experts, such as hospital episode statistics (HES), a nationally mandated dataset in English hospitals. This approach is error prone and is subject to variation in coding methodology at different hospitals and countries. By cross-referencing the data with the structured datasets generated by this tool, we can improve the accuracy and completeness of the information, unlocking deeper insights into patient care.
A more operational use case could involve the scheduling of further scans or treatment. The structured output produced by the tool could be fed into another model to automatically triage patients on hospital waitlists based on the severity of their conditions. This would ensure patients most at need of urgent care or at risk of deterioration are seen quickly.
AI in Dermatology: a White Paper by Edge Health for NHSE
The NHS is currently grappling with a growing demand for Dermatology. Waiting lists have grown by 82% since 2021, and the rate of GP referrals for skin cancer having nearly doubled in the last decade. This is compounded by a national shortfall in dermatologists as vacancies in 2021 amounted to 159 WTE. Our report, published in July 2024, has shown that AI holds considerable promise for skin cancer pathways including improving effectiveness and reducing wait times.
AI is currently in use for diagnosis within NHS skin cancer pathways with all lesions second-read by a clinician. Greater efficiency, speed of diagnosis and clinician time could be released if AI as a Medical Device (AIaMD) functioned autonomously. NHS England commissioned Edge health to conduct an independent review of the safety and effectiveness of AI in Dermatology and assessment of its performance against accepted standards of accuracy.
Methods and Key Findings
We examined real-world data from over 33,000 lesions assessed by DERM – an AIaMD developed by Skin Analytics, the only product that currently meets regulatory standards for autonomous use. We conducted a semi-systematic meta-analysis reviewing 153 studies and interviewed eight members of staff across three providers currently adopting the AIaMD. This enabled a grounded perspective on its application in skin cancer detection.
Our findings indicate that DERM’s diagnostic accuracy in ruling out melanomas is at least as good as in-person consultations with dermatologists. This suggests that AI could play a crucial role in distinguishing benign from concerning lesions, streamlining referrals, and ensuring those in need of urgent care are seen promptly. We also identified potential system-level efficiencies, finding that each pound spent could return up to £2.3 in savings. In this context, our report highlights AIaMD’s potential to refine the triage process, thereby addressing the rising demand for services and reducing waiting times for assessments.
While our economic analysis suggests potential savings, the primary focus of the report is on the clinical and operational implications of AIaMD, and what steps should be taken to monitor its use in Dermatology through post-market surveillance (PMS). Clear PMS plans and agreements need to be in place, with responsibilities lying with both deployment sites and manufacturers. Our report condenses PMS recommendations from several literature sources and offers an example of how PMS could be implemented in practice.
The report makes clear that the use of AI holds considerable promise for improving the efficiency and effectiveness of skin cancer pathways. Evidence of its deployment in the NHS has demonstrated that whilst the tool could be used autonomously to exclude benign skin, adequate safeguards, will need to be in place. This provides the potential to free up specialists to focus their expertise on the most urgent and complex cases.
Julia Schofield, Clinical Lead for Dermatology for the National Outpatient Recovery and Transformation programme
Read Our Report
The report concludes that thoughtful deployment of AI in Dermatology has the potential to enhance patient pathways and alleviate system pressures. With appropriate safeguards and continuous evaluation, AI can support the NHS in upholding its commitment to innovative, high-quality patient care.
AI-Teledermatology: Innovating Skin Cancer Diagnostics
The healthcare system in England and Wales is experiencing unprecedented pressure due to the sharp rise in demand for dermatology services. With one in four individuals seeking consultation for skin, hair, or nail conditions each year, the need for innovative solutions has never been greater. The COVID-19 pandemic exacerbated this strain, causing a 30% drop in dermatology appointments during 2020/21 and a subsequent surge in patient referrals post-pandemic, with suspected cancer referrals rising 13% nationally compared to 2018. Rising volumes of urgent suspected cancer referrals have significant impacts for system sustainability – under a strained system, they correlate with higher volumes of patients breaching care standards, such as the 62-day treatment standard, as explored in a previous piece of work.
The potential of teledermatology, particularly AI-powered teledermatology, has been recognised as a promising solution to expand service capacity and ensure equitable patient access to specialist care. The Skin Analytics AI-Powered teledermatology for Skin Cancer 2-week-wait (2WW) Pathway was pilot tested across University Hospitals of Leicester (UHL) sites starting from March 2022. This collaborative project was designed to respond to the local need for improved patient access to dermatology diagnostics and the achievement of 2WW cancer targets.
Our evaluation underscored the potential of AI-powered teledermatology. Despite being in its pilot phase, the AI tool demonstrated its capability to enhance patient access to dermatology services. While the initial benefit-cost ratio stood at 1.05, this figure doesn’t fully encapsulate the unquantified benefits, such as a reduction in biopsies, long-term care costs, and WLI clinics. Workforce costs were also front-loaded prior to capacity being fully utilised, leaving room for a higher benefit-cost ratio.
The current pathway model relies on second-reads to be performed on all AI-screened scans, with a further reduction in the potential benefit-cost ratio as well as increased pressure on clinical teams. In our evaluation, the AI outperformed documented clinical diagnostic standards[1], but our staff survey highlighted current reservations from consultants in dispensing of the second-reads altogether.
The evaluation also supported the health system through highlighting potential administrative challenges that scaled expansion would need to monitor for. These included timely booking of appointments for patients on the novel pathway, as well as ensuring that commissioning arrangements reflect the true costs of providing an innovative service – and are aware of the prospected savings.
Scenario Modelling for Future Savings
Looking ahead, we conducted scenario modelling to explore the potential for greater savings in the future. These scenarios hinge on reducing or removing the cost associated with the second read of dermoscopy images, leading to a benefit-cost ratio ranging from 1.3 to 1.9.
Our evaluation indicates that this novel pathway could be cost-effective in the long term. It could also offer considerable benefits to the wider Dermatology cohort, healthcare staff, and the health system if implemented at scale, with potential yearly savings across the Midlands ranging between £2.1M and £5.7M, depending on who performs the second read.
Recommendations for Enhancements
As part of our commitment to continuous improvement, we proposed several recommendations. These include streamlining administrative processes, evaluating the best option for lesion second reads and conducting further evaluations as the AI versions improve and more data becomes available.
Our work with Health Innovation East Midlands, UHL and Skin Analytics demonstrates Edge Health’s commitment to pioneering innovative healthcare solutions. Evaluating the effectiveness of new technologies such as AI-powered teledermatology is a fundamental step in improving services so that they are accessible, efficient, and patient-centred.
Our overall experience of working with Edge was very positive, and their analysis and evaluation process was robust and innovative. They handled challenges well and always sought a balanced solution with cross-stakeholder agreement. The Final Report was delivered on track and met the expectations outlined in the original scope and MOU.
Michael Ellis – Senior Innovation Lead, Health Innovation East Midlands
Key Successes
Conducted a comprehensive independent evaluation of the AI-powered teledermatology pilot initiative.
Identified potential for significant future savings through scenario modelling.
Proposed actionable recommendations to enhance the programme’s benefits and ensure long-term cost-effectiveness.
Highlighted the importance of considering administrative implications of implementing novel technologies.
Provided insights to guide future evaluations as AI technology evolves and more data becomes available.
This project was carried out in partnership with Health Innovation East Midlands
Full Report
The evaluation report can be accessed on the Health Innovation East Midlands website, as well as previewed below.
[1] Chuchu N, Dinnes J, Takwoingi Y, Matin RN, Bayliss SE, Davenport C, Moreau JF, Bassett O, Godfrey K, O’Sullivan C, Walter FM, Motley R, Deeks JJ, Williams HC. Teledermatology for diagnosing skin cancer in adults. Cochrane Database of Systematic Reviews 2018, Issue 12. Art. No.: CD013193.
Case study: Evaluating the benefits of integrating chemotherapy patient management apps
Challenges in the Existing Healthcare System for Chemotherapy Patients
Cancer patients undergoing chemotherapy have to navigate a complex healthcare system at a particularly stressful point in their lives. Various patient management apps exist to support both patients and providers with this treatment pathway. However, a lack of a single source of information disadvantages both patients and Trusts.
Integrated Solutions for Patient Management and Prescribing Process
In response to this, the industry leader in electronic chemotherapy prescribing developed a product that integrates all aspects of patient management from referral to discharge and simplifies the prescribing process for healthcare professionals. Additionally, another provider created a patient-facing mobile app that brings disparate pieces of information from across the healthcare ecosystem together and delivers personalized support for cancer patients.
A typical Trust will treat between 1,200 and 1,500 new patients with chemotherapy each year. As such there are significant benefits to integrating these two patient management solutions and offering a bundle for purchase by acute providers. Edge Health was commissioned to deliver a report on the potential impacts of the integration. Through a review of existing literature and clinical engagement, we assessed the wide range of benefits throughout the patient journey. By quantifying some of these benefits, we sought to highlight the potential magnitude of the advantages for both Trust’s finances and patients.
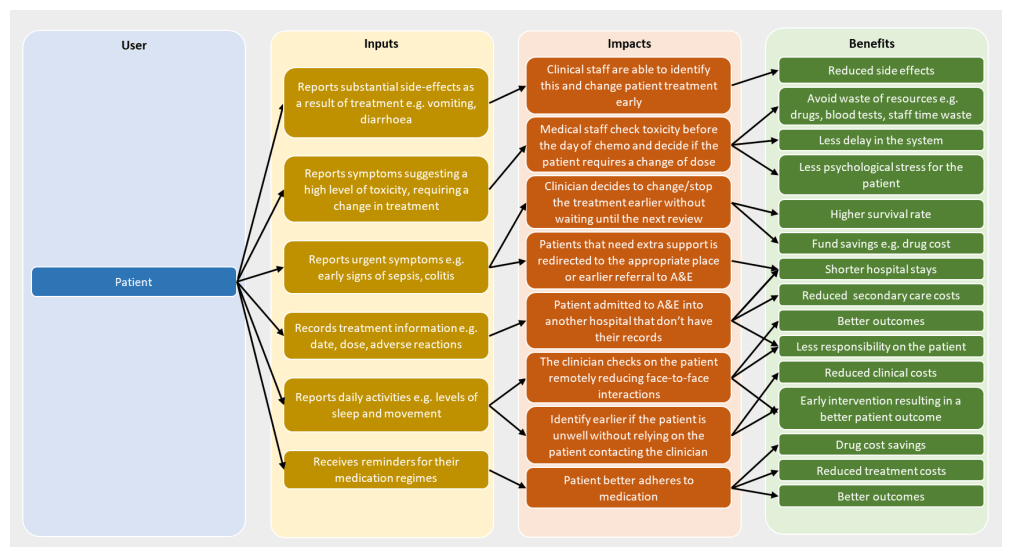
Our Analysis of Impacts and Benefits of patient management solutions
Positive Impacts on Patient Care and Risk Management
Many of the identified benefits are felt by the patients themselves. The integrated app and system facilitate the delivery of optimal patient care and minimise chemotherapy treatment’s risks and side effects. The advantages of this integration appear to be most material for patients who may require changes to their treatment, due to adverse reactions or toxicity, or for the rarer cases of more severe illnesses such as colitis and neutropenic sepsis.
Financial Benefits to the Healthcare System
There are also clear and direct financial benefits to the NHS. Chemotherapy drugs are expensive and waste is a substantial issue, whilst the costs of treating patients who develop more significant illnesses during their treatment can be very large. Through accurate capturing and sharing of patient-reported outcomes, the integration contributes to cost savings by minimising the expenses associated with treating such complications or illnesses.
The integration of chemotherapy patient management apps offers significant benefits to both patients and healthcare organizations. By streamlining the treatment process, improving patient care, and reducing financial burdens, this integrated solution has the potential to enhance the overall quality of care for cancer patients undergoing chemotherapy. Acute care providers can leverage these apps to optimize their treatment protocols and improve resource allocation, ultimately leading to better patient outcomes and more efficient healthcare delivery.
Technology can’t replace GPs (yet), but it can save them time
There has been an unprecedented focus in Primary Care to make better use of digital resources, providing virtual and remote consultations. Changing consultation modes will not provide the answers we need when looking at the growing GP workforce gap, which requires focussed planning on training, retention and addressing demand. We estimate that the benefit of innovation on workforce numbers will be relatively low compared to other strategies and that is by design – innovation should support, rather than replace, the workforce, though there is scope for potential productivity gains.
Closing the 2032 GP workforce gap, aiming for 8.5 % vacancy Number of GPs expressed as Full Time Equivalent (FTE)
With that in mind, we should not put innovation on the back burner, for at least two considerations. One, that discovering new ways of working relies on innovation, which may yet provide us with strategies to tackle need; secondly, that innovative ways of work can have ripple benefits on other areas, such as workforce and patient satisfaction and increase the potential to attract and retain doctors in primary care.
What’s out there?
Innovative solutions are widespread in Primary Care, and some have demonstrated promising changes the way healthcare is provided, particularly through bridging primary and secondary care, and making care more accessible. Consultant Connect, a service developed for North Central London CCG that allowed GPs to directly message specialists for advice and guidance, reduced secondary care referrals in 64% of contacts as specialists could provide advice to be implemented in primary care rather than requiring a referral.
The virtual boost promoted by compelling need during the pandemic has allowed e-consultations to flourish and transform the way time is spent in primary care: e-consultations in North London have allowed non-clinical queries to be directed to staff other than GPs, and GPs were able to deal with e-consultations much faster than in person, reducing face to face consultations by 25%.
Our previous work has highlighted the vast impact of video consultations beyond healthcare savings – such as savings on inpatient travel resulting in lower greenhouse gas emissions as well as £108m savings in lost productivity through avoiding 3m lost work hours.
Productivity gains through harnessing innovation can be very material – virtual consultations have saved PCNs approximately 17,200 hours – scaled nationally, this is equivalent to freeing enough capital to employ 900 GPs –, and eConsult has shown to reduce missed GP appointments by 60%, with large time and cost savings. These strategies could give a substantial boost to our 2032 workforce concerns, though it is important to recognise the technology supports and enables the workforce, it does not (yet) replace it.
How can innovation become a reality?
Innovating does not always equate to revolutionising systems – sharinglearning and making best use of resources in effective and innovative ways can be the best route to having a large impact. Working with Kaleidoscope and Cambridge and Peterborough STP, Edge Health supported the implementation of a digital first pathway for diabetic patients that enabled, through shared priorities and consistent approach to care, to improve care for diabetic patients and increase the uptake of the National Diabetes Prevention Programme without generating more work for GPs. Key to the success of the programme was the sharing of evidence that supported innovation within the STP, as well as the engagement with frontline staff that directly experienced the benefits of the innovative intervention.
We could draw four take home points from this successful implementation of innovation at scale:
Ideas should be generated locally, where need is clearly understood
Successful innovation relies on collaboration across practices – this promotes not only sharing of best practices, but also agreement on care delivery strategies that have the potential to level up working habits
Taking on from the example of practices, collaboration across ICBs will also enable effective innovation to reach other areas through cross-communication; central channels need to be available for this to happen
Innovation must involve frontline staff rather than be exclusively top-down, for effective implementation and longevity
The last consideration is particularly important in the context of workforce – attempting to implement innovative strategies will undoubtedly be a challenge amidst an overstretched, disenchanted workforce. Taking decisive steps towards tackling the workforce gap will be a necessary step to promote further innovation, and in return, innovation could hold the keys to better healthcare that makes best use of resources.
Evaluation of Eye Care Electronic Referral Systems
In 2017/18 ophthalmology outpatient activity was reported to be greater than any other NHS speciality. This high demand has been linked to the aging population, new treatments, eye conditions requiring multiple appointments a year, unwarranted variation in referrals, as well as a lack of discharge pathways for stable and lower risk patients. Demand-driven pressures on ophthalmic services have also risen further in the wake of the COVID-19 pandemic, and have been compounded by services suffering workforce supply challenges, with persistently low ophthalmologists per capita across the UK. It is, therefore, becoming increasingly important that processes to relieve pressure on ophthalmology services are developed and successfully deployed.
There has been growing interest in the potential benefits of using Eye Care Electronic Referral Systems (EeRS) and transfer of full volume scans/images in ophthalmology to improve pathways from primary care optometrists to specialist ophthalmologists in a Hospital Eye Service (HES). Through implementation of EeRS there is the hope that some of the pressures on both primary and secondary care could be alleviated.
Several pilots have been commissioned across the UK to test the use of EeRS, however, there remains a gap in the literature on the real-world benefits of this intervention. With expertise in both qualitative and quantitative research methods, Edge was commissioned to evaluate the use of one EeRS at the 6-month stage in its pilot. Interviews were held with optometrists, consultant ophthalmologists, optometry service delivery managers, clinical commissioners, optometry clinical technology managers and the EeRS provider, to understand the impacts that the technology could have on patient pathways. In parallel, cost data and CCG-level demand data were used to identify the potential cash and non-cash-releasing benefits to the system.
Quantitatively, it appears there have only been marginal cost and time efficiency gains. However, the pilot was in its infancy, and referrals and user sign-ups continued to grow month-on-month. Qualitatively, optometrist and ophthalmologist feedback suggested significant potential with many citing patients were seen quicker at HES, patients were more likely to be sent to the correct clinic for their first appointment, saving patient time and health system resources, as well as patients being less likely to get lost in the referral pathway.
This analysis also identified several next steps for the current pilot as well as key learnings for expansion and further roll-outs. These findings will be used to inform decisions makers on the real-world benefits of EeRS and help ensure future regional or national roll-outs have the data needed to deliver maximal benefit for the NHS.
In 2019, there were 748,000 people living with dementia in England. This population typically has complex care needs, placing considerable strain on the health and social care systems as well as on individuals themselves and their carers/families – at an estimated total cost to the UK of £37.4 billion a year.
Minder is a remote care platform that aims to improve the quality of life for people with dementia and their carers. It uses home sensors to detect an individual’s activity at home, and builds a model of ‘usual activity’ through use of artificial intelligence, allowing any deviations to be detected and flagged for follow-up, enabling early prevention. Minder has been developed by the research team at the UK DRI Care and Research Centre based at Imperial College London and the University of Surrey, in partnership with Surrey and Borders Partnership NHS Foundation Trust.
Recognising the benefits that Minder could have for people living with dementia, the UK DRI commissioned Edge Health to undertake a health economic evaluation of Minder. Through engagement with stakeholders and experts in the field, as well as review of existing evidence and literature, we built an understanding of the impacts that Minder could have on the health and social care systems, as well as on individuals with dementia and their carers. By modelling the costs associated with each of these impact pathways, we were able to estimate the Benefit Cost Ratio of Minder among the dementia population in England.
As part of their translation exercise, the UK DRI realised the need to have cost benefit figures at local population level. Through development of an adjustable model, enabling selection of specific geographies and dementia populations of interest, we were able to provide the UK DRI with a dynamic output demonstrating the value that Minder could bring for local populations, and the return on investment that could be made. This work will facilitate wider rollout of the technology in England, which if successful would allow a range of benefits to be realised across a large population of individuals, with huge benefits for health and social care systems.
“What many people don’t see if that AI is already part of the NHS… AI and other smart platforms are already helping us improve the services we deliver for the NHS, and ultimately, the individual’s patient experience” – fantastic coverage in The Mail on Sunday, featuring the DigitalHealth.London Accelerator and Edge Health! Read on!
”AI in the NHS Artificial intelligence is already being used across the UK. Gina Clarke looks at how it’s being implemented and the benefits to patients and practitioners. […]
SURGERY SCHEDULING: When it comes to planning surgical procedures, in order to minimise cancelled appointments, AI is helping NHS trusts such as South Tees to reduce waiting times. By using SpaceFinder, a product from Edge Health that can be implemented into existing software, the technology estimates how long a procedure will take and fits other surgeries accordingly — similar to the game Tetris. On average, up to two hours of operating time per theatre per day is currently unused, whereas this software can maximise the time. It also works to eliminate weekend procedures, which tend to cost more. However, it’s important to note that with the majority of today’s technology, humans still get the final say.”
Press release: Edge Health joins cohort 4 of the DigitalHealth.London Accelerator
Press release: Edge Health joins cohort 4 of the DigitalHealth.London Accelerator
Edge Health is proud to announce that it joins cohort 4 of the DigitalHealth.London Accelerator programme. The DigitalHealth.London Accelerator is a programme aimed at speeding up the development and scaling of digital innovations across health and care and pioneer their adoption by the NHS.
Across England, over 5 million people are waiting for an operation – almost as many people as there are in London. At the same time, hospital operating theatres often go unused due to poor scheduling. The complexity of modern scheduling requirements is not being met by the systems currently available in hospitals.
SpaceFinder is a software developed by Edge Health that uses advanced analytics to accurately predict operating times and propose optimal operating lists tailored to local conditions. These lists take account of all available information so that valuable theatre operating time is used effectively every day.
South Tees NHS Foundation Trust implemented SpaceFinder to put more activity into its core operating time. This allowed it to turn off weekend working. As well as being safer for patients, less frustrating for staff, it helped save £3 million. This innovative use of technology was well received by the CQC as “outstanding practice”.
Through DigitalHealth.London, Edge Health is looking to sped up the development and roll-out of SpaceFinder so that no patient ever must sit on a waiting list longer than needed.
 Back to News & Insights
Back to News & Insights